I broke up this Blog into three parts:
Part 1 focuses on her left leg - finding and fixing the leg muscle imbalances, adjusting the leg, ankle and foot, and releasing tight muscle
Part 2 focuses specifically on her right leg
Part 3 focuses on her low back and hip alignment, as well as posture, arch supports and strengthening exercises
HISTORY:
The patient is a 30-something year old female who presents with chronic left knee pain. I treated her right knee pain at the gym about a month ago, and the discomfort then moved to the left. She’s had it most of her adult life, though she became more aware of it over the past three years, and it’s gotten even worse over the past 6 months. It prevents her from taking long walks or hikes, lifting weights or even standing for long periods of time. She states that when she was a child, she used to do Mexican folk dancing where she would stomp on concrete in “yap heels,” and this may be where the initial trauma started.
ANKLE: Additionally, she twisted her right ankle yesterday stepping off a deck into a hole in the dirt. She "kind of" felt a pop, though her ankle didn't swell and is currently just sore. The patient points to the front of her right ankle and both inner shins
FEET: She has sensitive inner shins due in part to her flat feet.Knee: the patient points to the back of her left knee (called the Popliteal Fossa)
The patient’s feet collapse when she stands (loads), which is referred to as pronation.When I asked her to come into a deep supported squat, she tucks her hips, indicative of an overfiring ( hypertonic) low back muscles which are likely shutting down (inhibiting) the Glutes.
PART 3:
FINDINGS:
Alignment: Chiropractic Adjustments of the low back and hips:
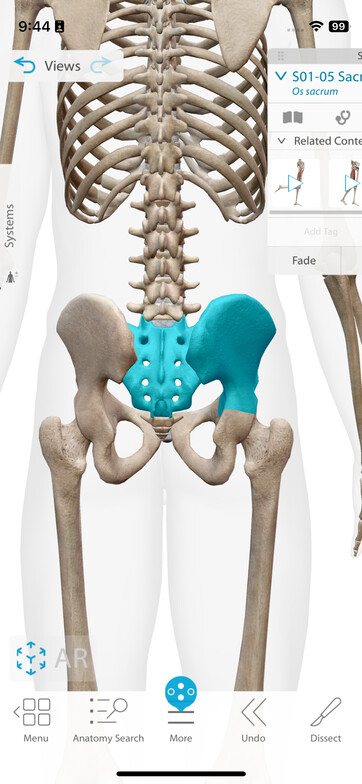
Adjustment at Pelvis: I assessed and adjusted the Sacro-Iliac Joint (SI joint) and Sacrum (the upside down triangular bone between both hip bones) with a drop table.The part of the table under the area being adjusted drops about 1" and adds more speed so that my hands doing the adjustment on the joint can put in less force.
Manual Therapy:
Dural release at Occiput: There is a sheath around the Spinal Cord called the Meninges. I think of it like the insulation around a wire. Except it's much more delicate and intricate. It allows Cerebral Spinal Fluid to circulate around the spinal cord. When there is tension in the system, this becomes a problem, and leads to physical ailments, stress and tension.
Postural Assessment:
COLLAPSED ARCHES: We assessed the loaded arch with the patient standing - her foot collapses when loaded, but in her case, her shoes helped to support her arches.
We discussed ways to modify an orthotic. We can add felt padding to raise the arch or support the forefoot, and we can also add material under the orthotic to make it stiffer so that it won’t collapse when loaded.
I also showed her exercises to strengthen her outer hips: this helps to engage and lift the arches.
“Monster Wobble” is one of my favorites, where the patient puts a circular rubber band around both ankles, keeping her feet parallel, and then shifts her weight from foot to foot, back and forth.
DISCUSSION:
REHAB:
Once the communication system is corrected, the muscles are repatterned and released and the joints are aligned, then it is appropriate to give the patient specific rehab exercises. In this case, I worked with her on two fronts: Posture in general and strengthening of the outer Glutes (lateral stabilization).
FLAT FEET:
I find that fallen arches often start at the pelvis. I had the patient practice standing with weight more towards her heels. If the toes start to come up, merely grab the ground with your toes. This is a nice exercise for the Plantar Fascia and flexor muscles of the foot.
Furthermore, Think about externally rotating your feet by turning them away from each other without actually moving your feet. This activates the outer hip muscles.
An extreme example of this is a dancer’s Plie. One exercise I gave the patient was to use a large rubber band around both ankles. Then I have her wobble by shifting weight to one then the other leg, slightly lifting each straight leg. All this while pressing the legs out to meet the band resistance. This is an excellent exercise for the outer hips.
CHIROPRACTIC:
The spine consists of 24 movable segments, the pelvis three. Each foot contains 26 bones - more than in the spine, and even one bone not moving properly will throw off the entire system.
The main ankle bone (the Talus) doesn’t have muscle attachments and if you roll it, it has trouble getting back into proper position. This will lead to muscles turning down or up to compensate and can lead to compensations and other misalignments all the way up the kinetic chain - to the knees, hips, to the low and even upper back and neck.
Chiropractic adjustments help improve function in the body. Chiropractic adjustments restore proper joint motion and correct misalignments in the spine and other joints. This realignment reduces nerve pressure, enhances nerve function, and improves communication between the brain and body. By addressing misalignments, chiropractic care also enhances overall mobility and joint functionality.
IN CONCLUSION:
If you read all three parts to this blog, you will understand how someone with knee pain can be helped by looking at all aspects of the system and not just where the pain is. There are even more areas I will likely address with this patient, including core strength and stability (we need this to walk and run), and even mind-body/ stress pohysiology - we store emotional memory in our body. I like to think of the body as the emotional cloud storage for the brain. Further assessment would likely branch out and show shoulder and elbow issues, since the walking / gait patterning involves swinging the opposite arms and legs. The more I look, the more I find, until things come together and the whole system hums along in harmony once again!