


The patient is a millenial female Crossfit athlete who presents with right shoulder, elbow & wrist pains that got worse doing pullups and boxing, which entail pulling and pushing movements.
This blog follows the attached treatment video, which is fairly long (22 minutes). To make it easier to follow, I’ve added (in parentheses) the video time so you can jump where you would like in the video.
A BIT OF DISCUSSION FIRST:
Muscle Physiology:
Chin-ups use an underhand grip, emphasizing the biceps and forearms, while pull-ups use an overhand grip, targeting the back and shoulders more. They both entail a fair amount of traction (hanging from a bar) whereas punching entails more compression (hitting a punching bag). All of this plays into what may be ailing my patient.
Concentric contractions occur when a muscle shortens while generating force, like during the upward phase of a bicep curl, as in actively doing a chin-up. Eccentric contractions involve the muscle lengthening under tension, as seen during the lowering phase of a bicep curl, as in lowering oneself down during a chin-up. Isometric contractions occur when a muscle generates force without changing length, like holding a plank or holding oneself in space mid chin-up.
“Save As”
The Deep Tendon Reflex (DTR) can be found in many parts of the body. The most commonly known is the tendon under the knee cap (think of Marcus Welby MD hitting your knee with a reflex hammer). But I prefer to use the tendon near the elbow. Shortening a tendon by lightly hitting it with a reflex hammer effectively acts like hitting Return on a keyboard. This stimulates the central nervous system, throwing it into a cross-crawl or Gait pattern, creating a “save as” or new “set point” for how these muscles are communicating with each other. This is a key tool used by P-DTR practitioners, thus the name of the technique (Proprioceptive Deep Tendon Reflex).
AND NOW ON WITH THE SHOW:
Treatment: First assessed and corrected the alignment of the shoulder and elbow.
Elbow: (2:15)
Next I tested the muscles around the elbow, which includes the upper and lower arm, and found some over-firing and some under-firing muscles. These muscles that move the bones, tendons connecting them to the bones, ligaments connecting bone to bone in each joint, and the connective tissues that lay over all of it like saran wrap - all of these structures are loaded with tiny receptor organs which pick up information in the area such as pressure, stretch and vibration. When stimulated, they fire off, sending information to the brain, which then interprets this information and sends back info to those muscles, in effect telling them what to do. What do muscles do? They essentially turn on and off. Not so much like a flip light switch, but more like a dimmer switch (partially on or off).
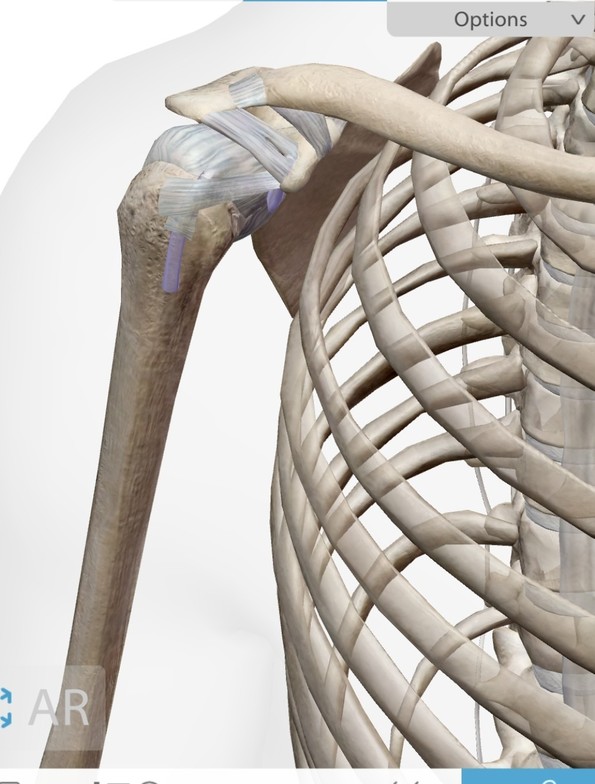
Shoulder: (3:30)
Once we fixed the elbow, I moved upstream to see where this kinetic dysfunction started. I found that one of the four shoulder stabilizers was under-firing (Subscapularis) and an opposite muscle was turning it down by over-firing (Infraspinatus). I found the proper receptors in each and provided the proper stimulation to each, followed by a deep tendon reflex (DTR) to reset the dysfunctional pattern between the two muscles.
Wrist: (7:09)
I found that when my patient’s hand was facing downward and in flexion, the muscles involved in that action weren’t working well. In this case, I found more elbow dysfunction affecting the wrist downstream. So I located the muscles both under and over firing to each other, found the dysfunctioning receptors, stimulated them and hit a DTR to reset them. I also found some other muscles then around the wrist that I also needed to reset. In the elbow I found a vibratory receptor and a pressure receptor and reset them.
Once I’ve reset the neurology around an area, then I can release the muscle with various myofascial techniques. I prefer to not do tissue work before correcting the neurology telling these muscles what to do.
In this case, I suspect a lot of the wrist and elbow issues are not from the gym but from typing! Low force repetitive movements that are not natural! (I demonstrate ART, Active Release Techique, 11:00-14:00)
NET (Neuroemotional Technique) (14:09)
I always also check if there’s a Mind-Body component to any dysfunction as well. The connective tissue is where we store emotion in the body. I think of the body as the Emotional Cloud Storage for the brain. In this case, I didn’t find anything, but this is described in detail in my other recent Blogs.
Alignment (15:05)
I next checked the alignment of the patient’s cervical spine (neck) using an electric impulse tool.I may also use an electric Percussor to release the fascial of the shoulder.
Lower Body: (17:30)
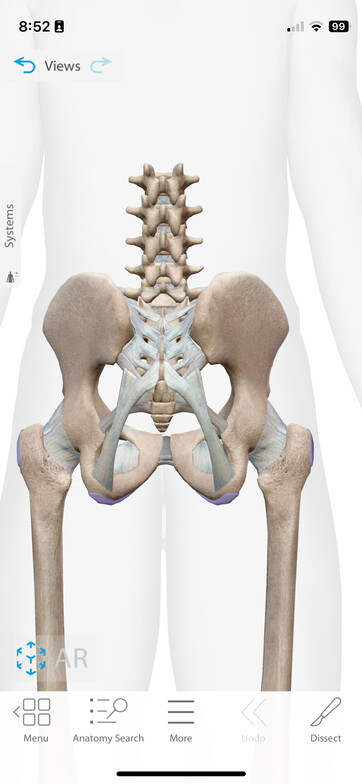
Everything is connected, so having corrected the neck and upper extremities, I may now move down to see what other parts of the body aren’t working well. In this case, I found an under firing right Glute. It is not uncommon that Glutes and shoulders dysfunction together. Think about what is happening when we walk - opposite legs and arms contract and relax. In this case the Glute is being shut down by an over-firing low back muscle group. In the same way, I determined the specific muscles, the exact part of each muscle and the specific receptors involved, in this case deep pressure & vibration. Then I can stimulate both and DTR (hit Return). The result is that the Gluteus now works properly.
I then check the alignment of the low back, sacrum and pelvis. I adjusted the thoracic spine. I also found a twist in the pelvis, which I helped to unwind using wedges (we call them blocks) to untwist. When there’s a torque in the pelvis, the body will often lock up the Thoracic spine to keep the sheath around the spinal cord (called the Meninges or Dura Mater) from twisting all the way up to the head.
Checking the Abs (21:51)I find that a lot of shoulder issues comes from the Core (abs), especially with runners, so I am checking this too. In this case, I didn’t find anything.
Summary:
We took a tour of the body to address all the related parts of a dysfunction which became apparent (pain) at the elbow. I find that this is the most effective way to truly correct a problem. Just focusing on the area that hurts is most often a bandaid at best.