



The patient is a young mother who severely sprained her right ankle a year ago jumping off a boat onto a dock. The injury was so severe at the time that she thought she had broken her ankle. However, she was overseas on a boat at the time so never got X-Rays or treatment.
She presents a year later able to walk but still gets knots in her calf. She is also currently breast feeding her baby, and thinks that Relaxin may be slowing the healing process.
Evaluation:
To evaluate the body, I am looking at movement patterns (sitting, bending...), ranges of motion of the spine and other joints of the body - in this case the ankle, the alignment of bones & joints, the strength and facilitation of muscles (are they able to fully lock when isolated and tested"?), and how these muscles respond to their opposite muscle, known as the antagonist. In order to move any joint in the body, one muscle needs to be able to release to that the opposite one can contract. This on-off relationship can get disrupted, leading to dysfunctional patterns in the body. I use PDTR to evaluate and correct these "short circuits" and have found that unless this is corrected, any further alignment, muscle release and rehab (lengthening or strengthening) will be slowed down.
Findings:
PDTR Concepts:
I like to think of muscles as lights and receptors as light switches. These receptors are throughout the body, in different parts of the muscles, tendons (where the muscle attaches to bone), ligaments (which hold bones together), and connective tissue or fascia (think of it as the saran wrap over all your muscles), as well as in the skin. There are two types of receptors - those for pain and those for position or motion.
I think of a dysfunctional pattern in the body, especially if it involves multiple muscles, like an old Western movie bar fight: it always starts with two, and then all the "extras" jump in and start throwing chairs. Likewise, any receptor dysfunction pattern starts with two (a primary and a secondary) and many other affected muscles will also turn "on" or "off" but fixing these won't fix the problem. The PDTR practitioner needs to be able to identify and correct the exact two main muscles in the exactly correct way in order to change that particular dysfunction. And the amazing thing is that when done right, this pattern is all but erased from the nervous system, like a reset.
PDTR Findings:
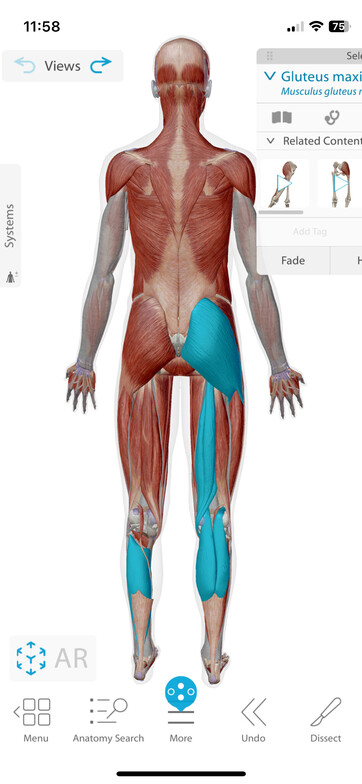
A Kinesiology & PDTR evaluation found multiple muscle imbalances in this region, including the following: an over-firing (hypertonic) right outer Calf muscle (Gastroc) and an under-firing (hypotonic) right inner Calf muscles (Gastroc), inner Hamstring, Soleus (deep calf muscle), and Glut Max (the butt muscle).
The outer Gastroc was being affected by a vibration receptor called a Meisner receptor, which is reactive to 256Hz. This muscle was reactive to a deep pressure receptor called a Pacini receptor in the Hamstring. The Gluteus and Soleus (deep calf muscle) went along for the ride, part of a larger compensation pattern.
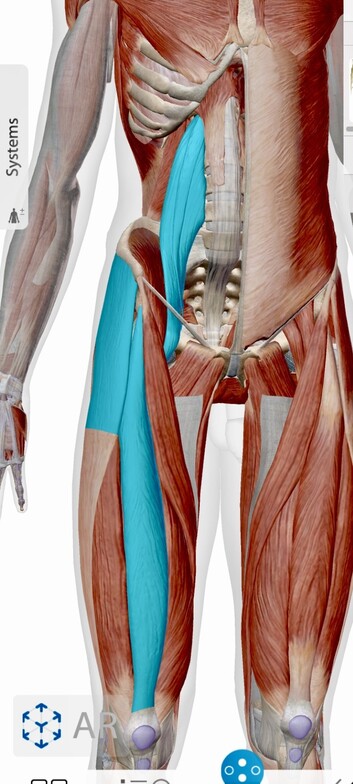
An over firing Right Gluteus Max with a Krauss vibration receptor with an under-firing Rt Psoas with a deep pressure receptor called a Pacini. Other related underfiring muscles include TFL, Rectus Femoris.
Pain receptors are deeper under the skin and also relay information to the brain which in turn affects muscle firing patterns. In this case, a pain receptor near the right Greater Trochanter (where your femor attaches to your hip) also inhibited muscles of the leg and hip.
Interestingly, I also found dysfunction in the left shoulder, in the SC joint where the shoulder attaches to the sternum, with a hypertonic pec and hypotonic Lat. Since gait incorporates opposite arm and leg swing, this may be part of her dysfunctional pattern.
Using PDTR, I was able to correct all of these dysfunctional pattern, resulting in normally firing muscles (normotonic)
Chiropractic Findings:
I adjusted the pelvis, using wedges to unwind a torque in the pelvis
Extremity Findings:
Anything outside of the spine is considered an extremity, such as the arms and legs. Extremity adjustments are an important part of chiropractic care and in this case
In this case, I adjusted the right lower leg: knee, ankle and foot, as well as the Lt SC joint (shoulder).
Follow up care:
Once muscle firing patterns are corrected, then it is much more effective to proceed with muscle-release care of tight muscles. For this I may use ART (Active Release Technique), Fascial Scraping using a beveled surgical steel tool to release fascia, as well as cupping and kinesiology taping.
Further Comments:
Our body is a scrap book of our lives, and we carry our traumas with us - structurally, biochemically and emotionally. In order to clear an injury, many pieces of a puzzle need to be addressed, much like needing all 6 digits to get into an iPhone!